The Host
Julie Rovner
KFF Health News
@jrovner
Read Julie’s stories.
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
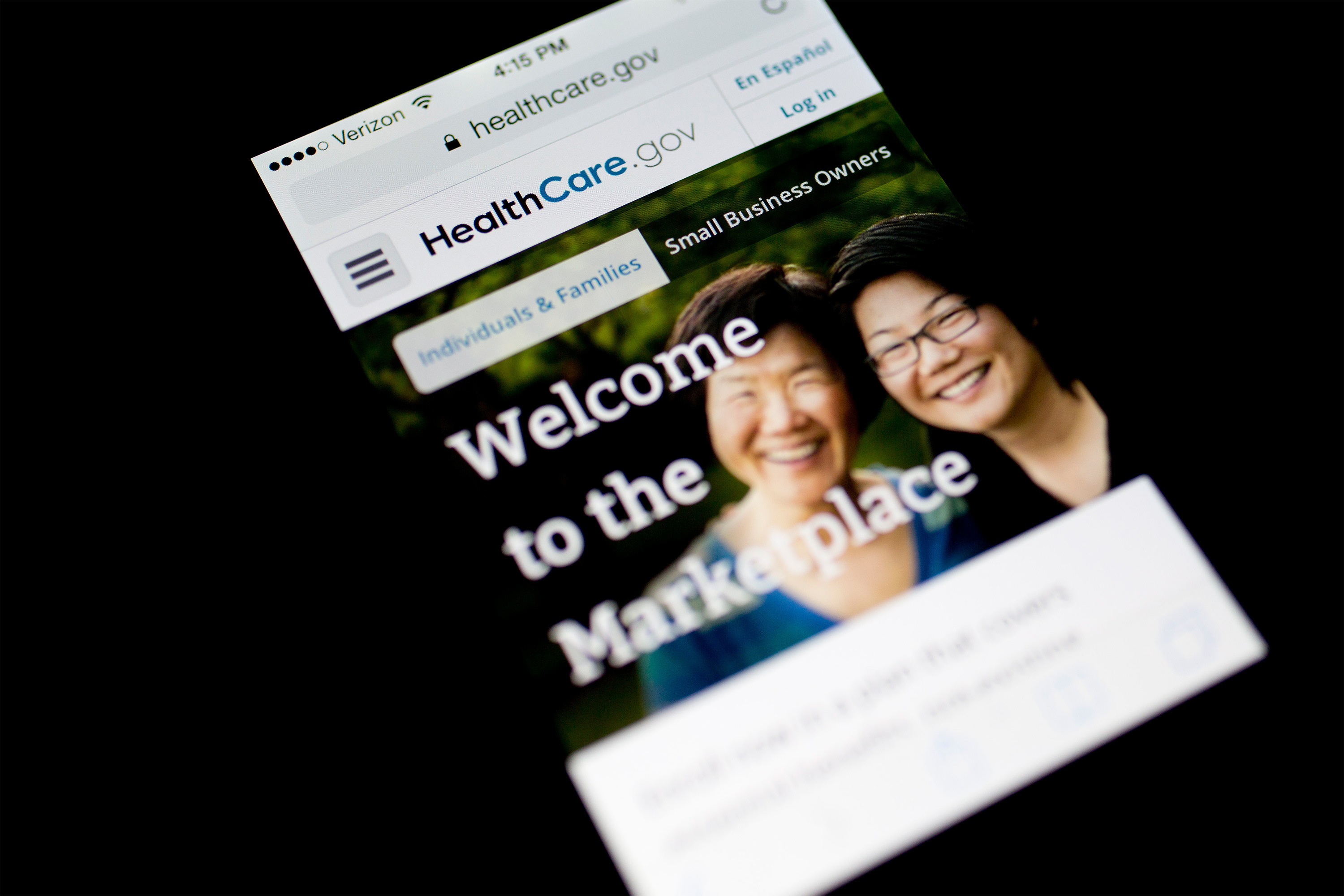
For the first time since 2004, it appears health insurance coverage will not be a central issue in the presidential campaign, at least judging from the first GOP candidate debate in Milwaukee Wednesday night. The eight candidates who shared the stage (not including absent front-runner Donald Trump) had major disagreements over how far to extend abortion restrictions, but there was not even a mention of the Affordable Care Act, which Republicans have tried unsuccessfully to repeal since it was passed in 2010.
Meanwhile, a new poll from KFF finds that health misinformation is not only rampant but that significant minorities of the public believe things that are false, such as that more people have died from the covid vaccine than from the covid-19 virus.
This week’s panelists are Julie Rovner of KFF Health News, Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico, Victoria Knight of Axios, and Margot Sanger-Katz of The New York Times.
Panelists
Joanne Kenen
Johns Hopkins Bloomberg School of Public Health and Politico
@JoanneKenen
Read Joanne’s stories
Victoria Knight
Axios
@victoriaregisk
Read Victoria’s stories
Margot Sanger-Katz
The New York Times
@sangerkatz
Read Margot’s stories
Among the takeaways from this week’s episode:
- The first Republican presidential debate of the 2024 cycle included a spirited back-and-forth about abortion, but little else about health care — and that wasn’t a surprise. During the primary, Republican presidential candidates don’t really want to talk about health insurance and health care. It’s not a high priority for their base.
- The candidates were badly split on abortion between those who feel decisions should be left to the states and those who support a national ban of some sort. Former Vice President Mike Pence took a strong position favoring a national ban. The rest revealed some public disagreement over leaving the question completely to states to decide or advancing a uniform national policy.
- Earlier this summer, Stanford University’s Hoover Institute unveiled a new, conservative, free-market health care proposal. It is the latest sign that Republicans have moved past the idea of repealing and replacing Obamacare and have shifted to trying to calibrate and adjust it to make health insurance a more market-based system. The fact that such plans are more incremental makes them seem more possible. Republicans would still like to see things like association health plans and other “consumer-directed” insurance options. Focusing on health care cost transparency could also offer an opportunity for a bipartisan moment.
- In a lawsuit filed this week in U.S. District Court in Jacksonville, two Florida families allege their Medicaid coverage was terminated by the state without proper notice or opportunity to appeal. It seems to be the first such legal case to emerge since the Medicaid “unwinding” began in April. During covid, Medicaid beneficiaries did not have to go through any kind of renewal process. That protection has now ended. So far, the result is that an estimated 5 million people have lost their coverage, many because of paperwork issues, as states reassess the eligibility of everyone on their rolls. It seems likely that more pushback like this is to come.
- A new survey released by KFF this week on medical misinformation found that the pandemic seems to have accelerated the trend of people not trusting public health and other institutions. It’s not just health care. It’s a distrust of expertise. In addition, it showed that though there are people on both ends — the extremes — there is also a muddled middle.
- Legislation in Texas that was recently signed into law by Republican Gov. Greg Abbott hasn’t gotten a lot of notice. But maybe it should, because it softens some of the state’s anti-abortion restrictions. Its focus is on care for pregnant patients; it gives doctors some leeway to provide abortion when a patient’s water breaks too early and for ectopic pregnancies; and it was drafted without including the word “abortion.” It bears notice because it may offer a path for other states that have adopted strict bans and abortion limits to follow.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week they think you should read, too:
Julie Rovner: KFF Health News’ “Doctors and Patients Try to Shame Insurers Online to Reverse Prior Authorization Denials,” by Lauren Sausser.
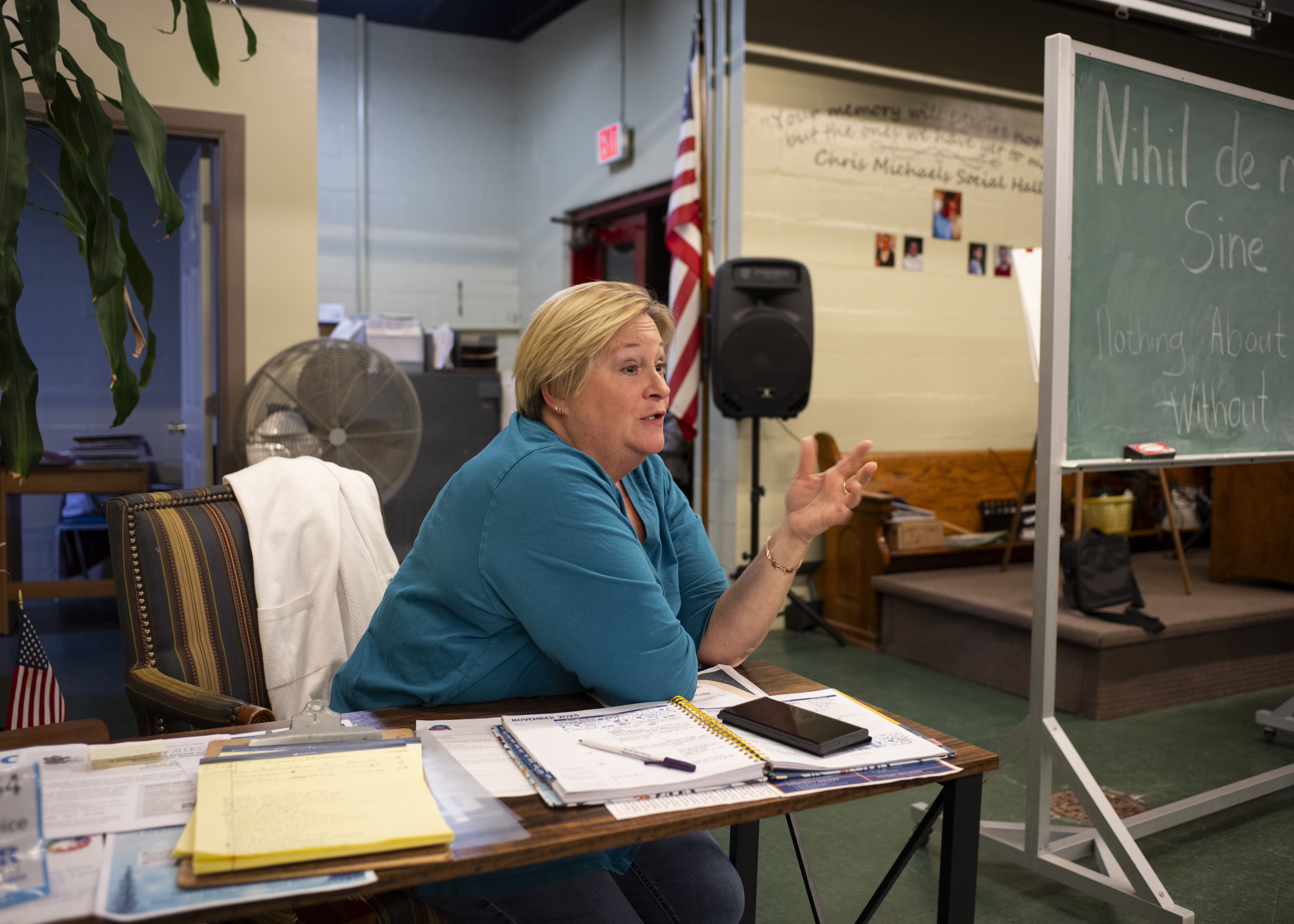
Margot Sanger-Katz: KFF Health News’ “Life in a Rural ‘Ambulance Desert’ Means Sometimes Help Isn’t on the Way,” by Taylor Sisk.
Joanne Kenen: The Atlantic’s “A Simple Marketing Technique Could Make America Healthier,” by Lola Butcher.
Victoria Knight: The New York Times’ “The Next Frontier for Corporate Benefits: Menopause,” by Alisha Haridasani Gupta.
Also mentioned in this week’s episode:
Click to open the transcript
Transcript: A Not-So-Health-y GOP Debate
[Editor’s note: This transcript, generated using transcription software, has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News. And I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, Aug. 24, at 10 a.m. As always, news happens fast, and things might have changed by the time you hear this. So, here we go. We are joined today via video conference by Margot Sanger-Katz of The New York Times.
Margot Sanger-Katz: Good morning.
Rovner: Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico.
Joanne Kenen: Hi, everybody.
Rovner: And Victoria Knight of Axios News.
Victoria Knight: Hello, everyone.
Rovner: No interview this week, but we’ll have an entire interview episode next week. More on that later. First, we will get to this week’s news. Well, Wednesday night saw the first Republican presidential debate of the 2024 cycle, minus front-runner Donald Trump, in what could only be called a melee, on Fox News Channel. And while there was a spirited debate about abortion, which we’ll get to in a minute, I didn’t hear a single word about anything else health-related — not Medicare or Medicaid, nor any mention of the Affordable Care Act. Was anybody surprised by that? For the record, I wasn’t. I wasn’t really expecting anything except abortion.
Kenen: Well, somebody, I think it was [former New Jersey Gov. Chris] Christie actually pointed out that nobody was talking about it.
Knight: Mike Pence. It was [former Vice President] Mike Pence, actually.
Kenen: Oh, Pence. OK. “Nobody’s talking about Medicare and Social Security.” And then he didn’t talk about it, and nobody mentioned the ACA.
Rovner: Is the ACA really gone as a Republican issue, for this cycle, do we think?
Kenen: Well, I think it’s become, like, a guerrilla warfare. Like, they’re still trying to undermine it. They’re not trying to repeal it, but they’re looking at its sort of soft underbelly, so to speak, and trying to figure out where they can put more market forces on, which we can sort of come back to later. But they spent 10 years trying to repeal it, and they just figured out what they’ve got to do now is pretend it’s not there. Right now, abortion is their topic.
Rovner: Well, let us turn to that.
Sanger-Katz: Yeah, I was just going to say that we’ve been seeing this happen a little bit over the last couple of cycles. In the 2020 race — I went through the transcripts of all of the speakers during the Republican National Convention and was really staggered by how few mentions of Obamacare there were relative to the way that the issue had been discussed in the past. But I think — just a note, that this is the Republican debate. Republicans don’t really want to be talking about health insurance and health care, because they don’t really have affirmative plans to put forward and because I think that they see that there are some real political liabilities in staking out a strong position on these issues. But in a general election, I think it will be impossible for them to avoid it, because, I think, Joe Biden has a lot of things that he wants to say. I think he is very committed to, in particular, broadcasting that he wants to protect Medicare. I think he’s quite proud of the expansions that he’s made of the Affordable Care Act. And so, this is a little bit of a weird moment in the race because, you know, we really only have one party that’s having a primary, and its leading candidate is not participating in the debates. And so, I think these candidates are trying to focus elsewhere. But it is — I will say, as someone who’s covered a couple of these now — it is a weird experience to have health care and health policy feel like a second-tier issue, because it was so central — Obamacare, in particular — was just so central to so many of these election cycles and such an animating and unifying issue among Republican voters, that this kind of post-failure-of “repeal and replace” era feels very different.
Kenen: One really quick thing is, they’re going to hit Biden on inflation. Economically, it’s his most vulnerable point, and health care costs are a burden. And I was a little surprised, without going into Obamacare and repeal and all that stuff, they mentioned the price of food, the price of gas, they mentioned interest rates and housing. It would have been really easy, and I expect that at some point they will start doing it, to talk about the cost of health care, because Biden’s done a huge amount on coverage and making insurance more affordable and accessible. But the cost of health care, as we all know, is still high in America.
Rovner: And at very least, the cost of prescription drugs, which has been a bipartisan issue going back many, many years. All right. Well, the one health issue that, not surprisingly, did get a lot of attention last night was abortion. With the exception of Mike Pence, who has been an anti-abortion absolutist for his entire tenure in Congress, as governor of Indiana, and as vice president, everyone else looked pretty uncomfortable trying to walk the line between the very anti-abortion base of the party and the recognition that anti-abortion absolutism has been a losing electoral strategy since the Supreme Court overturned Roe last year. What does this portend for the rest of the presidential race and for the rest of the down-ballot next year? Rather than trying to bury the fact that they all disagree, they all just publicly disagreed?
Knight: And I think they also, like, if you listened, [former U.S. ambassador to the United Nations] Nikki Haley kind of skirted around how she would address it. She talked about some other things, like contraception and saying that there just weren’t enough votes in the Senate to pass any kind of national abortion ban. [Florida Gov.] Ron DeSantis also, similarly, said he was proud of his six-week bill but didn’t quite want to answer about a national abortion ban. There were the few that did say, like, Hey, we’re into that. And some said, You know, it needs to go back to the states. So there definitely was kind of this slew of reactions on the stage, which I think just shows that the Republican Party is figuring out what message, and they don’t have a unified one on abortion, for sure.
Rovner: I do want to talk about Nikki Haley for a second, because this is what she’s been saying for a long time that she thinks that there’s a middle ground on abortion. And, you know, bless her heart. I’ve been covering this for almost 40 years and there has never been a middle ground. And she says, well, everybody should be for contraception. Well, guess what? There’s a lot of anti-abortion stalwarts who think that many forms of contraception are abortion. So there isn’t even a consensus on contraception. Might she be able to convince people that there could be a middle ground here?
Sanger-Katz: Oh, what I found sort of interesting about her answers: I think on their face they were kind of evasive. They were like, I don’t need to answer this question because there’s not a political consensus to do these things. But I do think it was sort of revealing of where the political consensus is and isn’t that I think she’s right. Like, realistically, there aren’t the votes to totally ban abortion; there aren’t the votes to renew the Roe standard. And I think she was in some ways very honestly articulating the bind that Republicans find themselves in, where they, and I think a lot of their voters, have these very strong pro-life values. At the same time, they recognize that getting into discussions about total abortion bans gives no favors politically and also isn’t going to happen in the near future. So, I felt like, as a journalist, you know, thinking about how I would feel having asked her that question, I felt very dissatisfied by her answer, because she really didn’t answer what she would like to do. But I do think she channeled the internal debate that all these candidates are facing, which is, like, is it worth it to go all the way out there with a policy that I know will alienate a lot of American voters when I know that it cannot be achieved?
Rovner: I was actually glad that she said that because I’ve been saying the opposite is true also — everybody says, well, why didn’t, you know, Congress enshrine abortion rights when they could have? The fact is, they never could have. There have never been 60 votes in the Senate for either side of this debate. That’s why they tried early after Roe to do national bans and then a constitutional amendment. They could never get enough votes. And they tried to do the Freedom of Choice Act and other abortion rights bills, and they couldn’t get those through either. And this is where I get to remind everybody, for the 11,000th time, the family planning law, the Title X, the federal Family Planning [Services and Public Research] Act, hasn’t been reauthorized since 1984 because neither side has been able to muster the votes even to do that. Sorry, Joanne, you wanted to say something.
Kenen: No, I thought Haley’s response on abortion was actually really pretty interesting on two points, right? She didn’t technically answer the question, but she also said this question is a fantasy — you know, face it. And, you know, she said that, and then she mentioned the word contraception. She did not dwell on it. She sort of said it sort of quickly. She missed an opportunity, maybe, just for one or two more sentences. You know, she said we need to make sure that contraception … she’s the only woman on that stage. She’s a mother; she’s got two kids. And, you know, there is uncertainty. After Dobbs there were advocacy groups saying, you know, they’re going to ban contraception tomorrow, and that didn’t happen. And we still don’t know how that fight will play out and what types of contraception will be debated. But I noticed that she said that on a stage full of Republicans, and I noticed that nobody else — all men — didn’t pick up on it.
Rovner: The big divide seemed to be, do you want to leave it completely to the states or do you want to have some kind of national floor of a ban? And they seemed, yeah —
Kenen: Yeah, and the moderators didn’t pick up on that. I mean, there was such a huge brouhaha on the stage. You know, the moderators had a lot of trouble moderating last night. It wouldn’t have been easy for them to get off of abortion and follow up on contraception. But I thought it was just sort of an interesting thing that she noted it.
Sanger-Katz: I will say also, and I agree with Julie: With the possible exception of Mike Pence, even the candidates that were endorsing some kind of national abortion policy, we’re talking about a 15-week gestational limit. There really wasn’t anyone who was coming out and saying, “Let’s ban all abortions. Let’s even go to six weeks,” which many of the states, including Florida, have done. So I do think, again, like, even the candidates that were more willing to take an aggressive stand on whether the federal government should get involved in this issue were moderating the position that you might have expected for them before Dobbs.
Kenen: But even 15 weeks shows how the parameters of this conversation have changed, because what the Republicans had been doing pre-Dobbs was 20 weeks, with their so-called fetal-pain bills. So 15 weeks, which would have sounded extremely radical two years ago — compared to six weeks, 15 sounds like, oh, you know, this huge opportunity for the pro-choice people. And it is another sign of how this space has shrunk.
Sanger-Katz: Yeah, no, I don’t mean that it’s a huge opportunity for the pro-choice people, but I think it reflects that even the candidates who were willing to go the most out on the limb in wanting to enforce a national abortion restriction understand the politics do not permit them to openly advocate going all the way towards a full ban.
Rovner: While we are on the subject of Republicans and health, there actually is a new Republican plan to overhaul the health system. Sort of. It’s from the Hoover Institution at Stanford, from which a lot of conservative policy proposals emanate. And it’s premised on the concept that consumers should have better control of the money spent on their health care and a better idea of what things cost. Now, this has basically been the theme of Republican health plans for as long as I can remember. And the lead author of this plan is Lanhee Chen, who worked for Republicans in the Senate and then led presidential candidate Mitt Romney’s policy shop, and whose name has been on a lot of conservative proposals. But I find this one notable more for its timing. Republicans, as we mentioned, appear to have internalized the idea that the only thing they can agree on when it comes to health care is that they don’t like the Affordable Care Act. Is that changing or is this just sort of hope from the Republican side of the policy wonk shop?
Sanger-Katz: I think this is connected to the discussion that we had about the debate, but it feels to me like we are in a bit of a post Obamacare era where the fights about “Are we going to continue to have Obamacare or not?” have sort of faded from the mainstream of the discussion. But there’s still plenty of discussion to be had about the details. The Democrats clearly want to expand Obamacare in various ways. Some of those they have done in a temporary fashion. Others are still on the wish list. And I think this feels very much like the kind of calibration adjustment, you know, small changes, tinkers on the Republican side to try to make the health insurance market a little bit more market-based. But this is not a big overhaul kind of plan. This is not a repeal-and-replace plan. This is not a plan that is changing the basic architecture of how most Americans get their insurance and how it is paid for. This is a plan that is making small changes to the regulation of insurance and to the way that the federal government finances certain types of insurance. That said, I think the fact that it’s more incremental makes it feel like these are things that are more likely to potentially happen because they feel like there are things that you could do without having a huge disruptive effect and a big political backlash and that you could maybe develop some political consensus around.
Rovner: It does, although I do feel like, you know, this is a very 2005 plan. This is the kind of thing that we would have seen 15 years ago. But as Democrats have gotten the Affordable Care Act and discovered that the details make it difficult, Republicans have actually gotten a lot on the transparency side and, you know, helping people understand what things cost. And that hasn’t worked very well either. So there’s a long way to go, I think, on both sides to actually make some of these things work. Victoria, did you want to add something?
Knight: Yeah, I’ve been talking to Republicans a lot, trying to figure out like what is their next go-to going to be. And I think they’re pretty understanding that ACA is set in place, but they still don’t want to give up that there are alternative types of health insurance that they want to put out there. And I think that seems that’s kind of what they realize they can accomplish if they get another Republican president and they’re going to try to do association health plans again. They’re going to try to expand some of these what they call health reimbursement arrangements, things like that, to just like kind of try to add some other types of health insurance options, because I think they know that ACA is just too entrenched and that there’s not much else they can do outside of that. And then, yeah, I think focus a little more on the transparency and cost because they know that’s a winning message and that is the one thing in Congress right now on the health care end that seems to have bipartisan momentum for the most part.
Rovner: Yeah, I think you’re absolutely right. Well, another issue that could have come up in last night’s debate but didn’t was the unwinding of Medicaid coverage from the pandemic. The news this week is that the first lawsuit has been filed accusing a state of mistreating Medicaid beneficiaries. The suit filed against Florida by the National Health Law Program and other groups is on behalf of two kids, one with a disability, and a mom who recently gave birth. All would seem to still be eligible, and the mom says she was never told how to contest the eligibility determination that she was no longer eligible, and that she was cut off when she tried to call and complain. State officials say their materials have been approved by the Centers for Medicare & Medicaid Services, which they have, and that Florida, in fact, has a lower procedural disenrollment rate than the average state, which is also true. But with 5 million people already having been dropped from Medicaid, I imagine we’re going to start to see a little more pushback from advocacy groups about people who are, in all likelihood, still eligible and have been wrongly dropped. I’m actually a little surprised that it took this long.
Kenen: Many of the people who have been dropped, if they’re still eligible, they can get recertified. I mean, there’s no open enrollment season for Medicaid. If you’re Medicaid-eligible, you’re Medicaid-eligible. The issue is, obviously, she didn’t understand this. It’s not being communicated well. If you show up at the hospital, they can enroll you. But people who are afraid that they aren’t covered anymore may be afraid of going to the hospital even if they need to. So there’s all sorts of bad things that happen. In some of these cases, there are simple solutions if the person walks in the door and asks for help. But there are barriers to walking in the door and asking for help.
Rovner: I was going to say one of the plaintiffs in this lawsuit is a child with a disease …
Kenen: Cystic fibrosis.
Rovner: Right. That needs expensive drugs and had not been able to get her drugs because she had been cut off of Medicaid. So there’s clearly stuff going on here. It’s probably true that Florida is better than the average state, which means that the average state is probably not doing that well at a lot of these things. And I think we’re just starting to see, you know, it’s sort of mind-numbing to say, oh, 5 million people have been separated from their health insurance. And again, we have no idea how many of those have gotten other health insurance, how many of those don’t even know and won’t know until they show up to get health care and find out they’re no longer covered. And how many people have been told they’re no longer covered but can’t figure out how to complain and get back on?
Sanger-Katz: And it’s this very extreme thing that’s happening right now. But it is, in many ways, the normal system on steroids. You know, if you’ve been covering Medicaid for any period of time, as all of us have, like, people get disenrolled all of the time from Medicaid for these administrative reasons, because of some weird hiccup in the system, they move, their income didn’t match in some database. This is a problem that a lot of states face because they have financial incentives often to drop people off of Medicaid because they have to pay a portion of the cost of providing health care. And a lot of them have rickety systems, and they’re dealing with a population that often has unstable housing or complicated lives that make it hard for them to do a lot of paperwork and respond to letters in a timely way. And so part of the way that I’ve been thinking about this unwinding is that there’s a particular thing that’s happening now, and I think there’s a lot of scrutiny on it, appropriately. And I think that there should be to make sure that the states are not cutting any corners. But I also think in some ways it’s sort of like a way of pressure-testing the normal system and reminding us of all of the people who slip through the cracks in normal times and will continue to do so after this unwinding is over. And these stories in Florida, to me, do not feel that dissimilar from the kinds of stories that I have heard from patients and advocates in states long before this happened.
Rovner: Yeah, I think you’re right. It’s just shining a light on what happens. I mean, it was the oddity that they were … states were not allowed to redetermine eligibility during the pandemic because normally states are required to redetermine eligibility at least once a year. And I think some do it twice a year. So it’s, you know, these redeterminations happen. They just don’t happen all in a huge pile the way they’re happening now. And I think that’s the concern.
Sanger-Katz: And it also, I think, really shines a light on the way that Medicaid is structured, where the Affordable Care Act simplified it quite a lot because, [for example], you’re in an expansion state and you earn less than a certain amount of money, then you can get Medicaid. But there are all of these categories of eligibility where, you know, you have to be pregnant, you have to be the parent of a child of a certain age. You have to demonstrate that you have a certain disability. And I think [it] is a reminder that this is a pretty complicated safety net, Medicaid. You know, there’s lots of things that beneficiaries have to prove to states in order to stay eligible. And there’s lots of things, honestly, you know, if states really want to make sure that they are reserving resources for the people who need them, that they do need to be checking on. And so I think we’re all just sort of seeing that this is a messy, complicated process. And I think we’re also seeing that there are these gaps and holes in who Medicaid covers. And it’s not the case that we have a perfect and seamless system of universal coverage in this country. We have this patchwork and people do fall between the cracks.
Kenen: And this is one of the most vulnerable populations, obviously. Some of the elderly are also very vulnerable, but these are people who may not speak either English or Spanish. They don’t have access to computers necessarily. I mean, we’re giving the least assistance to the population that needs the most assistance. And, you know, I mean, I think if Biden wanted to be really savvy about fixing it, he’d come out with some slogan about “Instead of Medicare unwinding, it’s time to have Medicare rewinding,” or something like that, because they’re going to have to figure … I mean, they have taken some steps, but it’s a huge mess, and the uninsurance rate is going to go up, and hospitals are going to have patients that are no longer covered, and it’s not going to be good for either the health care system or certainly the people who rely on Medicaid.
Rovner: I think it’s noteworthy how much the administration has been trying not to politicize this, that apparently, you know, we keep hearing that they won’t even tell us which states, although you can … people can sort of start to figure it out. But, you know, states that are having a more difficult time keeping eligible people on the rolls, shall we say, when the administration could have … I mean, they could be trumpeting, you know, which states are doing badly and trying to shame them. And they are rather very purposely not doing that. So I do think that there’s at least an attempt to keep this as collegial, if you will, as possible in a presidential election year. So my colleagues here at KFF have a depressing, but I guess not all that surprising, poll out this week about medical misinformation and how much of the public believes things that simply aren’t true — like that more people died from the covid vaccine than covid itself, or that ivermectin is a useful treatment for the virus. It’s not. It’s for parasites. And the survey didn’t just ask about covid. People have been exposed to, and a significant percentage believe, things like that it’s harder to get pregnant if you’ve been on birth control and stop. It isn’t. Or that people who keep guns in their house are less likely to be killed by a gun than those who don’t. They’re not. But what’s really depressing is the fact that the pandemic seems to have accelerated an already spiraling trend in distrust of public institutions in general: government, local and national media, and social media. Are we ever going to be able to start to get that back? I mean, you know, we talk about the woes with public health, but this goes a lot deeper than that, doesn’t it?
Kenen: And it’s not just health care. When you look at historical metrics about trust — which I’ve had to for a course I teach — we were never a very trusting society, it turns out. We’ve had large sectors of the population haven’t been trusting of many institutions and sectors of society for decades. We’re just not too huggy in this country. It’s gotten way worse. And what you said is right, but it’s broad. It’s not just doctors. It’s not just vaccines, it’s expertise. This distrust is really corrosive. But of all the things in that survey, one that really blew me away was we’re like, what, 13 years since Obamacare was passed? Only 7% or 8% — “only,” I should say only in quotes, you know — only 7% or 8% still thought there were death panels, but something like 70% wasn’t sure if there were death panels. Like, has anyone known anyone who went before a death panel? Since 2010? And yet 70% — I mean, I may be a little off, I didn’t write it down — but it’s something like 70% weren’t sure. And that is a mind-blowing number. It just says, you know, they weren’t ready to come out and say, yes, there are death panels. But that meant that a lot of Democrats also weren’t sure if there were death panels There are no death panels.
Knight: I was just gonna say, I also thought it was interesting that it showed people do use social media to get a lot of their information, but then they also don’t trust the information that they get on there. So it’s kind of like, yeah …
Rovner: And they’re right not to!
Knight: Yeah, they’re absolutely right not to. But then it’s also like, well, they’re then just not getting health information at all, or if they’re getting it, they just don’t trust it. So just showcasing how difficult it is to fill that void of health information, like, people just aren’t getting it or don’t trust it.
Rovner: I feel like some of this is social literacy. I mean, you know, we talk about health literacy and things that people can understand, but, you know, people don’t understand the way journalism works, the difference between the national news and what you see on Facebook. And I think that’s, Joanne, going back to your point about people not trusting expertise, it’s also not being able to figure out what expertise is and who has expertise. I mean, that’s really sort of the bottom line of all this, isn’t it?
Kenen: Well, I mean, I was doing some research — I can’t remember the exact details, this was something I read several months ago — but there was one survey maybe a couple of years ago where the majority of people said they don’t trust the news they read, but they’re still getting their news from something that they don’t trust. So it sounds sort of funny, but it’s actually not. I mean, it’s really a crisis of people don’t know what to believe. The uncertainty is corrosive, and it’s health care and politics, this widening chasm of people with alternative sets of facts — or alternative worldviews, anyway. So it’s not good. I mean, it was a really good survey, it was a really interesting survey, but some of it wasn’t so surprising. I mean, that there’s still people who, like, the fertility issues and the vaccines. You can sort of understand why those have lingered in the environment we’re in. I had actually had a conversation the other day with a political scientist who had studied the death panel rumors 10 years ago. And I said, what about now? And, you know, he was sort of … he hadn’t looked at it and he was sort of saying, well, you know, there aren’t any. And people have probably figured that out by now. Well, no. I have to email him the study, right?
Sanger-Katz: Anytime that I read a study like this, I am also reminded — and I think it is useful for all of us to be reminded of this and probably most people who are listening to the podcast — that the average American is just not as tuned in on the news and on the Washington debate and on the minutia of public policy, as all of us are. So, you know, and I think that that is part of the reason why you see so many people not sure about these things. It’s clearly the case that they are being exposed to bad information and that is contributing to their uncertainty. And I think the rise of misinformation about both health policy and about actual, you know, health care, in the case of covid, is a bad and relatively newer phenomenon. But I also think a lot of people just aren’t paying that close attention, you know, and it’s good to be reminded of that.
Kenen: The book I just read that I referred to — it’s by an MIT political scientist named Adam Berinsky, and it’s called “Political Rumors.” And it just came out, and he was talking about exactly that, that we’re all exposed to misinformation. We can’t avoid it. It’s everywhere. And that for people who aren’t as engaged with day-to-day politics, they end up uncertain. That’s this messy middle, which they also use in the KFF survey. They came up with a very similar conclusion about the “muddled middle,” I think was the phrase they used. And what this political scientist said to me the other day was that, you know, pollsters tend to not look at the “I don’t know, I’m uncertain, no opinion.” They sort of shunt them aside and they look at the “yes” or “no” people. And he was saying, no, no, no, you know, this is the population we really need to pay attention to, the “Uncertains” because they’re probably the ones you can reach more. And in the real world, we saw that with vaccination, right? I mean, in the primary series — I mean, booster takeup was low — but in the primary when there was a lot of uncertainty about the vaccines, the people who said “no way I am ever going to get the vaccine” — I mean, KFF was surveying this every month — most of them didn’t. You know, a few on the margins did, but most of them who were really militantly against the vaccine didn’t take it. The ones who were “I don’t know” and “I’m a little scared” and “I’m waiting and seeing” … a lot of them did take it. They were reached. And that’s sort of an important lesson to shift the focus as we deal with distrust, as we deal with disinformation and we deal with messaging, which is good, and truth-building and confidence-building, it is that muddled middle that’s going to have to be more of a target than we have traditionally thought.
Rovner: Well, in the interest of actually giving good information, we have a couple of updates on the reproductive health front. For those of you keeping score, abortion bans took effect this week in South Carolina and Indiana after long drawn-out court battles. Meanwhile, in Texas, an update to our continuing discussion of women with pregnancy complications who’ve been unable to get care because doctors fear running afoul of that state’s ban, a couple of weeks ago, reports Selena Simmons-Duffin at NPR, Texas Gov. Greg Abbott very quietly signed a law that created a couple of exceptions to the ban for ectopic pregnancies and premature rupture of membranes, both of which are life-threatening to the pregnant woman, but just not necessarily immediately life-threatening. I had not heard a word about this change in the law until I saw Selena’s story. Had any of you?
Kenen: In fact, it should have come up because of this court case in Texas about, you know, a broader health exception — it’s not even “health,” it’s life-threatening. It’s like, at what point do you get sick enough that your life is in danger as opposed to, you know, should you be treating that woman before … you see what direction it’s going, and you don’t let them go to the brink of death? I mean, that was the court case and Abbott fought that. But yeah, it was interesting.
Rovner: It was a really interesting story that was also, you know, pushed by a state legislator who was trying very hard not to … never to say the word abortion and to just make sure that, you know, this was about health care and not abortion. It’s an interesting story, we will link to it.
Sanger-Katz: I wonder if other states will do this as well. It seems like, as we’ve discussed, you know, abortion bans are not as popular as I think many Republican politicians thought they would [be]. And I do think that these cases of women who face really terrible health crises and are unable to get treated are contributing to the public’s dislike of these policies. And on the one hand, I think that there is a strong dislike of exceptions among people who support abortion bans because they don’t want the loopholes to get so big that the actual policy becomes meaningless. On the other hand, it seems like there is a real incentive for them in trying to fix these obvious problems, because I think it contributes to bad outcomes for women and children. And I think it also contributes to political distaste for the abortion ban itself.
Kenen: But it’s very hard to legislate every possible medical problem … I mean, what Texas did in this case was they legislated two particular medical problems. And some states … they have the ectopic — I mean, ectopic is not … there’s no stretch of the imagination that that’s viable. Right? The only thing that happens with an ectopic pregnancy is it either disintegrates or it hemorrhages. I mean, the woman is going to have a problem, but making a list of “you get this condition, you can have a medical emergency abortion, but if you have that condition and your state legislator didn’t happen to think about it, then you can’t.” I mean, the larger issue is: How do you balance the legal restrictions and medical judgments? And that’s … I don’t think any state that has a ban has completely figured that out.
Rovner: Right. And we’re back to legislators practicing medicine, which is something that I think the public does seem to find distasteful.
Sanger-Katz: I mean, I don’t think that this solves the problem at all, but I think it does show a surprising responsiveness to the particular bad outcomes that are getting the most publicity and a sort of new flexibility among the legislators who support these abortion bans. So it’s interesting.
Rovner: All right. Meanwhile, another shocking story about pregnant women being treated badly. The Centers for Disease Control and Prevention reported this week that a survey conducted this April found that 1 in 5 women reported being mistreated by medical professionals during pregnancy or delivery. For women of color, the rate was even higher: more than 1 in 4. Mistreatment included things like getting no response to calls for help, being yelled at or scolded, and feeling coerced into accepting or rejecting certain types of treatment. We know a lot of cases where women in labor or after birth reported problems that went ignored. Among the most notable, of course, was tennis legend Serena Williams, who gave birth to her second child this week after almost not surviving the birth of her first. We’re hearing so much about the high maternal mortality rate in the U.S. What is it going to take to change this? This isn’t something that can be solved by throwing more money at it. This has got to be sort of a change in culture, doesn’t it?
Kenen: No. I mean, it’s … if someone who’s just given birth, particularly if it’s the first time and you don’t know what’s normal and what’s not and what’s dangerous and what’s not dangerous, and, you know, it’s a trauma to your body. I mean, you know, I had a very much-wanted child, but labor is tough, right? I always say that evolution should have given us a zipper. But the philosophy should be, if someone who’s just been through this physical and emotional ordeal, has discomfort or a question or a fear, that you respect it and that you calm it down, you don’t dismiss it or yell at somebody. When you’re pregnant, you read all these books and you go to Lamaze workshops and you learn all this stuff about labor and delivery. You learn nothing about what happens right after. And it’s actually quite uncomfortable. And no one had ever told me what to expect. And I didn’t know. And I always, like, when younger women are having babies, I let them know that, you know, talk to your doctor or learn about this or be prepared for this, because that is a really vulnerable point. And that this survey — and it’s more Black and poor women, and Latina women in this survey, it’s not that … it’s disproportionate like everything else in health care — they’re being disrespected and not listened to. And some of them are going to have bad medical outcomes because of that.
Rovner: As we are seeing. All right. Well, that is this week’s news now. We will take a quick break. Then we will come back and do our extra credit.
Hey, “What the Health?” listeners: You already know that few things in health care are ever simple. So if you like our show, I recommend you also listen to “Tradeoffs,” a podcast that goes even deeper into our costly, complicated, and often counterintuitive health care system. Hosted by longtime health journalist and my friend Dan Gorenstein, “Tradeoffs” digs into the evidence and research data behind health care policies and tells the stories of real people impacted by decisions made in C-suites, doctors’ offices, and even Congress. Subscribe wherever you get your podcasts.
OK, we’re back. It’s time for our extra-credit segment. That’s when we each recommend a story we read this week we think you should read too. As always, don’t worry, if you missed it; we will post the links on the podcast page at KFFHealthNews.org and in our show notes on your phone or other mobile device. Victoria, why don’t you go first this week?
Knight: So my extra credit is from The New York Times, and the story is called “The Next Frontier for Corporate Benefits: Menopause.” It basically details how a lot of companies are realizing that, you know, as more women get into leadership positions, high-level leadership, executive positions, they’re in their 40s, late 40s, early 50s, that’s when menopause or perimenopause starts happening. And that’s something that can last for a while. I didn’t realize the stories, that it can last almost 10 years sometimes. And so it was talking about how, you know, it affects women for a long period of time. It can also affect their productivity in the workplace and their comfort and being able to accomplish things. And so they were realizing, you know, we kind of need to do something to help these women stay in these positions. And there was actually an interesting tidbit at the very end where it was talking about some companies may even be, like, legally compelled to make accommodations. And that’s due to the new Pregnant Workers Fairness Act, which says that employers have to provide accommodations for people experiencing pregnancy but also related medical conditions. They’re saying menopause could be included in that. And just some of the benefits some of these companies were offering were access to virtual specialists, but they were talking about, like, if they need to do other things like cooling rooms and stuff like that. So I thought it was kind of interesting. And another employer benefit that maybe some employers are thinking about adding.
Kenen: I think all offices should have, like, little nap cubicles and man-woman, pregnant-not pregnant. And, you know, just like “life is rough.” [laughter]
Knight: I agree.
Kenen: Just a little corner!
Rovner: Joanne, why don’t you go next?
Kenen: Mine is from The Atlantic. It’s by Lola Butcher. And it is “A Simple Marketing Technique Could Make America Healthier.” And it’s basically talking about how some medical practices are doing what we in the news business and the tech industry knows of as “A-B testing.” You know, a tech company may try a big button or a little button and see which one consumers like. Newsrooms change headlines— headline A, headline B and see which one draws more readers — and that hospitals and medical practices have been trying to do. In some cases, it’s text messaging two different kinds of reminders to figure out, you know … one example was the message with something like 78 characters got women to book a mammogram, but a message with 155 characters did not. Two text messages were better than one for booking children’s vaccines. So some people are very excited about this. It’s getting people to do preventive care and routine care. And some people think this is just not the problem with health care, that it’s way deeper and more systemic and that this isn’t really going to move the needle. But it was an interesting piece.
Rovner: Any little thing helps.
Kenen: Right. This was an interesting piece.
Rovner: Margot.
Sanger-Katz: I wanted to talk about an article in KFF Health News from Taylor Sisk. The headline is “Life in a Rural ‘Ambulance Desert’ Means Sometimes Help Isn’t on the Way,” and it’s a really interesting exploration of some of the challenges of ambulance care in rural areas, which is a topic that is near and dear to my heart. Because when I was a reporter in New Hampshire covering rural health care delivery, I spent the better part of a year writing about ambulance services and the challenges there. And I think this story is highlighting a real challenge for people in these communities. And I think it’s also really a reminder that the ambulance system is this weird, off-to-the-side part of our health care system that I think is often not well integrated and not well thought of. It tends to be regulated as transportation, not as health care. It tends to be provided by local governments or by contractors hired by local governments as opposed to health care institutions. It tends to have a lot of difficulty with billing a very high degree of surprise billing for its patients, and also just a real lack of health services research about best practices for how fast ambulances should arrive, what level of care they should provide to people, and on and on. And I just think that it’s good that she’s highlighted this issue. And also, I think it is a reminder to me that ambulances are probably worth a little bit more attention from reporters overall.
Rovner: Well, my story is also something that’s near and dear to my heart because I’ve been covering it for a long time. It’s from my KFF Health News colleague Lauren Sausser. It’s called “Doctors and Patients Try to Shame Insurers Online to Reverse Prior Authorization Denials.” And it is a wonderful 2023 update to a fight that Joanne and I have been covering since, what, the late 1990s. It even includes comments from Dr. Linda Peeno, who testified about inappropriate insurance company care denials to Congress in 1996. I was actually at that hearing. The twist, of course, now is that while people who were wrongly denied care at the turn of the century needed to catch the attention of a journalist or picket in front of the insurance company’s headquarters. Today, an outrage post on Instagram or TikTok or X can often get things turned around much faster. On the other hand, it’s depressing that after more than a quarter of a century, patients are still being caught in the middle of appropriateness fights between doctors and insurance companies. Maybe prior authorization will be the next surprise medical bill fight in Congress. We shall see. All right. That is our show for the week. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review; that helps other people find us, too. Special thanks, as always, to our amazing engineer, Francis Ying. Also, as always, you can email us your comments or questions. We’re at [email protected]. Or you can tweet me or X me or whatever. I’m @jrovner, also on Bluesky and Threads. Joanne?
Kenen: I am also on Twitter, @JoanneKenen; and I’m on Threads, @joannekenen1; and Bluesky, JoanneKenen.
Rovner: Margot.
Sanger-Katz: I’m @sangerkatz.
Rovner: Victoria.
Knight: I’m @victoriaregisk on X and Threads.
Rovner: Well, we’re going to take a week off from the news next week, but watch your feed for a special episode. We will be back with our panel after Labor Day. Until then, be healthy.
Credits
Francis Ying
Audio producer
Stephanie Stapleton
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ ‘What the Health?’ on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.